A new pricing survey into Tanzania’s heroin market shows that heroin use has spread far inland from the coastal ‘southern route’, and the quality of heroin for sale reveals surprising inland supply routes.
In recent years, quantities of heroin smuggled along the East and Southern African coast have increased considerably. While most of the heroin shipped from Afghanistan along this so-called ‘southern route’ is destined for consumer markets in Europe, a significant local heroin trade and consumer market have developed, transforming what was initially understood to be a coastal transit trade into an integrated regional drug economy.1 Although it is difficult to quantify with certainty how the East African heroin market has expanded, it is clear that it now extends beyond the seaboard region. This is evident from a number of sources: the increased rates of seizures reported at the national level; reporting from regional law enforcement and civil society working on reducing the harms associated with drug use; growing reports of increasing heroin routes across neighbouring states, such as Botswana,2 Swaziland,3 the Democratic Republic of the Congo, Malawi and Zambia,4 and the South African interior provinces;5 and, more broadly, an increase in reported injecting drug use across sub-Saharan Africa.
Why collect drug prices?
However, there is little granular information available on the spectrum of drug markets across the East and Southern African region, and particularly on drug prices and forms of sale outside of urban centres. To fill this data gap, the Global Initiative Against Transnational Organized Crime (GI-TOC) is carrying out surveys on regional drug use markets and drug prices, so as to track the types of drugs consumed, methods of consumption, the consumer base for local markets and illicit drug prices. Preliminary results of these surveys from Tanzania shed light on the relationships between heroin supply, quality and price, and may give indications of which regions in Tanzania’s national heroin economy are linked through supply chains, and which regions diverge. These initial results are illustrated in the map (Figure 1).
Data was collected in partnership with a local civil- society organization affiliated with people who use drugs. Domestic heroin retail price data was gathered through field interviews conducted with heroin users and market dealers active in 15 drug market sites across the country. These locations include urban, peri-urban and rural geographies, and represent the majority of the administrative regions of the country. Owing to significant security concerns, it was not possible to collect sufficient data in locations bordering with Mozambique, including the regions of Mtwara, Ruvuma and Lindi. Metrics addressing retail price range (minimum to maximum) in local currency, user perception of product quality, and local market demand and supply characteristics were gathered for each site. A photograph was taken of representative heroin retail samples from most locations for reference, and for representation of retail packaging characteristics. The sample photos and price points illustrated in the map are representative of the most common retail sample available in that location and the mean retail price point for that sample. While data continues to be reviewed by the GI-TOC, some initial findings of the field research exercise can be drawn out.
Our initial results show that there is no place in Tanzania where heroin is not available. The reported domestic retail price of heroin in Tanzania ranges between TZS2 000 and 8 000 (equivalent to €0.79–3.15) per dose, with a mean price of TZS4 000 (€1.57).The average number of doses taken by a heroin user in a day fluctuates significantly across the country, from six to 20 or more doses in urban and peri-urban areas, while higher amounts were recorded in rural areas. Situational factors, such as price, perceived dose purity and method of consumption (heavier users who inject heroin – as opposed to smoking or inhaling – tend to consume more), shape the daily amount of heroin consumed.
The price of heroin does not appear to be correlated closely with its perceived quality. Pricing seems more closely related to supply-related factors, such as the consistency of its availability in particular local markets. For example, relatively high prices are being paid for heroin of very poor quality in places such as Mwanza and Kigoma, with dealers and users reporting that the heroin available in such distant rural locations is cut down repeatedly with a variety of adulterants that muddy its appearance, mute its effect and, in some cases, give its liquid form a glutinous consistency, which makes it difficult to inject. Overall, injection of heroin is an increasingly common method of use in rural areas, following a trend seen in urban areas for some years.
On quality, our initial results seem to show that the further away the heroin is acquired from a large urban centre, such as Dodoma or Dar es Salaam, the lower its perceived quality. Both these cities are reported to be geographic cornerstones for the distribution of heroin throughout the country, where mid- and low- level domestic trafficking groups receive heroin from international supply networks before transporting it to local markets for sale.
The price of heroin in more remote areas is reportedly determined, in part, by dealers passing on the costs of transport and supply to users. There appear to be no secure, organized supply pipelines in such areas. Dealers in remote areas rely on local entrepreneurs with links to the illegal market, who arrange heroin shipments from primary suppliers either in Dodoma or Dar es Salaam. Shipment is arranged either through people carrying the drug on public transport or through small caches hidden in commercial vehicles. The heroin that is procured for these remote locations is already cut at source. In some cases, the heroin supplied from Dodoma or Dar es Salaam is prepackaged in small single dose packets for retail; in others, it is purchased in larger wholesale quantities to be cut again by rural suppliers before being distributed locally.
The retail packaging of heroin provides interesting information about forms of consumption and about heroin supply routes. The majority of retail doses are sold as a ‘pinch’, whereby the adulterated heroin is packaged in a narrow polypropylene tube that is heat-sealed at each end (as seen in the images of doses acquired in Dar es Salaam, Morogoro and Singida – see Figure 1). A major difference in appearance between pinches in different locations is in the colour of the contents. Darker colours tend to indicate higher levels of adulteration. The quantity and quality of heroin in a pinch vary according to location. For example, in some places, a pinch may be slightly larger in size and appear to contain more product, but, according to users, this is because the quality of the pinch material is lower as a result of repeated cutting, and dealers increase the weight as a means of accounting for a decrease in purity. This presents a challenge in trying to determine the volumes of local heroin supply and demand, as it is not possible to determine a universal national measure for the number of pinches per gram.
Our sample results from Dodoma, Mwanza and Mbeya showed a strong similarity in retail packaging, which suggests that these three markets are closely linked through a single supply chain. In some locations, however, there is a distinct difference in packaging of retail heroin doses. For example, on the Zanzibari island of Unguja, heroin is distributed in distinct, curly-tailed foil packaging, a marked difference from most of the mainland markets.
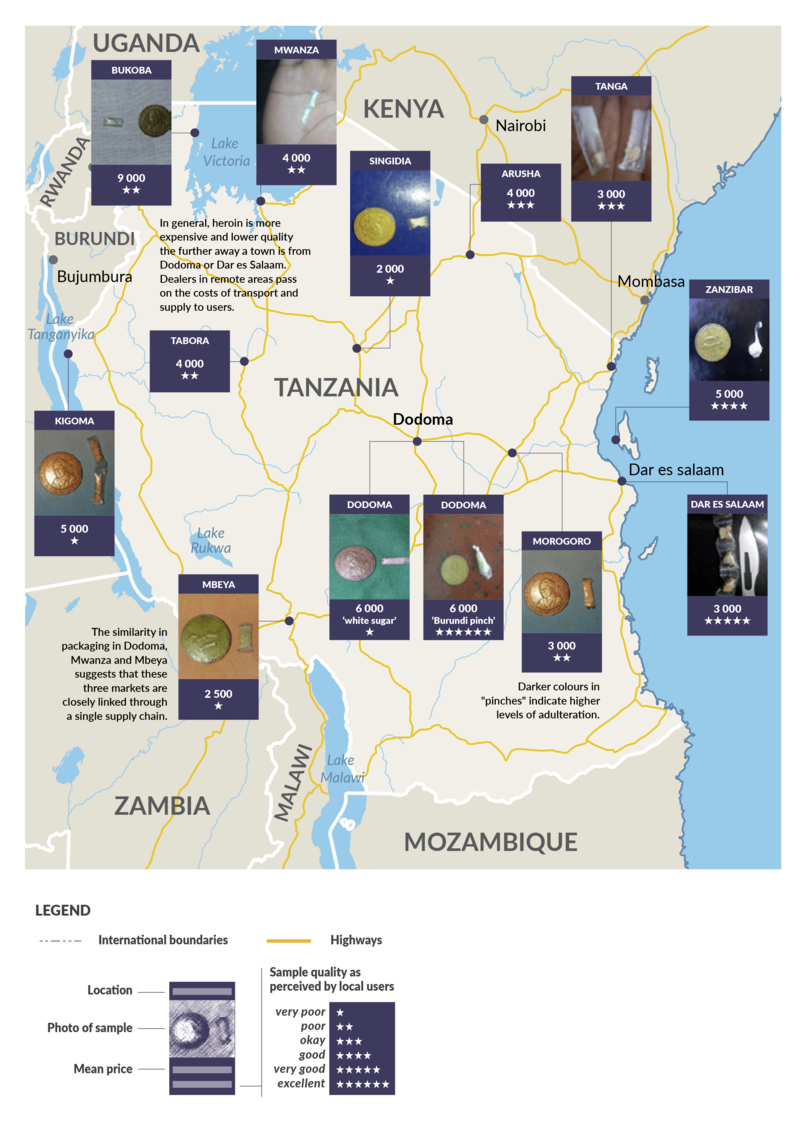
Figure 1 How a countrywide heroin market is supplied by several transnational routes; drug prices and perceived quality in Tanzania
In Dodoma, there is a second type of retail dose available known as a ‘Burundi pinch’, which in its packaging is different from the regular pinches – it is sold in a small polyethylene ‘twister’ (as pictured) and is reportedly of much higher quality than the other more regular pinches. This has spawned copycat production of pinches in Dodoma, which are sold as ‘Burundi pinches’, but which contain mostly white powdered adulterant, and little heroin by volume. Such apparent deviations in packaging most likely signify supply chains that are outside of, or tangential to, the existing domestic network. Interviews with dealers appear to support this conclusion as, in terms of the Dodoma market, a hitherto undefined supply channel entering Tanzania overland from Burundi, with origins in the overland trafficking of heroin from the major airports of Tanzania’s eastern African neighbours, was described by several informants.
Few discrete, fixed flows
These results provide new and important information about how local drug markets function. But they also confirm that the picture is substantially more complicated than we previously believed. The survey data from Tanzania, as well from ongoing interviews across the region, suggest that when it comes to local markets, there are few fixed flows of heroin that can be identified and blocked. Rather than following distinct streams, the supply of heroin is more akin to a shallow flood. The decades of impunity that traffickers have enjoyed mean that there are now multiple entry points into the regional market, and many competing or concurrent channels of supply, interwoven with the physical landscapes. The heroin is distributed with different levels of purity, volume and regularity, and the market is run by groups and networks of various sizes. The fact that heroin is supplied with significantly different levels of purity to the same retail consumers, and at the same price, is a symptom of a domestic heroin market with few barriers to entry for aspiring traffickers and dealers.
Notes
-
Simone Haysom, Peter Gastrow, and Mark Shaw, the heroin coast: A political economy along the East African seaboard, ENACT, June 2018, https://enactafrica.org/research/research-papers/the-heroin-coast-a-political-economy-along-the-eastern-african-seaboard. ↩
-
Megan Cox and Mukendi Kayembe, ‘An unusual tourist. A case of a body packer’s death in Botswana’, African Journal of Emergency Medicine, 5:e9-e10, 2015. ↩
-
Dlamini Gugu and Makondo Davison, The prevalence of drug and substance use among school-going teenagers in the Shiselweni region of Swaziland, International Journal of Innovation and Applied Studies, 20(2): 652–660, 2017. ↩
-
Jenny Tiberio et al, Context and characteristics of illicit drug use in coastal and interior Tanzania, International Journal of Drug Policy, 51: 20–26, 2018. ↩
-
Andrew Scheibe et al, HIV prevalence and risk among people who inject drugs in five South African cities, International Journal of Drug Policy, 30: 107–115, 2016. ↩